Digital radiography is the new technology that's found most often in U.S. dental schools, while CAD/CAM denture fabrication and hard-tissue lasers were the technologies least likely to be taught in the schools, according to a new study.
Researchers found that the technology implementation rates for dental schools generally followed the rate of acceptance within private practices. The authors of the study, which was published in the Journal of Dental Education, argued that the continued exposure to new technologies is critical to the future success of dentistry students (J Dent Educ, March 2015, Vol. 79:3, pp. 259-264).
"Especially considering the high cost of dental education, incorporating new technologies into the curriculum gives students a greater return on their academic investment -- one that will ultimately affect their future practices and patient care," they wrote. "This exposure improves the quality of the curriculum by keeping students current with the rest of the dental community during dental school and for the rest of their careers."
CAD/CAM, tissue lasers lag in adoption
The researchers emailed an online survey to the deans of all 62 U.S. dental schools in early 2013. The survey asked whether 12 specific dental practice technologies were being incorporated into their programs, including CAD/CAM software, digitally aided orthodontic appliances, and cone-beam CT (CBCT).
“Incorporating new technologies into the curriculum gives students a greater return on their academic investment -- one that will ultimately affect their future practices and patient care.”
The researchers received 33 usable survey responses, for a 52% response rate. According to the survey findings, digital radiography was the most implemented technology, with an 85% penetration rate. Rotary endodontics closely followed digital radiography with an 81% penetration rate.
CAD/CAM denture fabrication and hard-tissue lasers were least likely to be taught in schools, with penetration rates of 20% and 24%, respectively. Nevertheless, the schools' incorporation of newer technologies tended to follow the same acceptance rates found in private practice. The authors found only one exception -- CBCT.
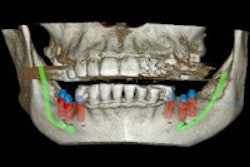
CBCT had a high penetration rate within dental school curricula, but the systems are not commonly found in private practices. The authors argued that this could be because CBCT equipment is expensive, and universities can more likely afford the cost than practices. However, dentists still regularly rely on imaging with CBCT.
"Since dental practitioners do routinely send patients to imaging centers for CBCT diagnostics in implant treatment planning, learning about this technology while in dental school is useful," they wrote.
Newer schools are early adopters
The researchers also took into account whether the institutions were publicly or privately funded, the age of the program, and each program's geographic location. They found that dental schools more than 60 years old were less likely to have incorporated emerging technologies than newer programs.
The researchers suggested that implementation rates may vary because older schools have established policies and curricula. On the other hand, newer schools are generally more willing to accept changes within the field and, consequently, will more readily change their course content.
They also found that dental schools with class sizes of more than 100 students were less likely to incorporate emerging technologies. This may be because schools with a larger number of students require more resources, financially or otherwise, to incorporate newer devices, they noted.
However, the researchers found no significant differences in the implementation of technologies among schools in different geographic locations or those that were publicly and privately funded, which went against their initial hypothesis.
Students need to know about new technologies
One of the biggest challenges with implementing new technology into dental schools is preparing the faculty, the study authors noted. Because most dental school faculty come from clinical environments, the majority of training resources instruct faculty about teaching methodologies, techniques, and advancements, as opposed to educating them about emerging technologies.
In addition, faculty must coordinate their course content to provide students with a consistent learning environment, which may also explain the slower acceptance and integration of new technologies into dental school curricula.
However, the study authors urged dental schools not to become complacent with teaching students about new technologies. They stressed that schools must teach students how to use and learn about new dental technologies while in school and once they graduate to ensure their alumni's long-term success.
"As the field of dental medicine continues to incorporate new technologies, dentists must stay current by participating in continuing education courses and reading and analyzing the appropriate literature," the authors concluded. "Dental educators must also stay current with emerging technologies as they are developed and implemented in order to provide the most comprehensive education to their students."