A panoramic x-ray scan revealed bilateral osteolytic lesions in a man's jaw, leading to the diagnosis and treatment of the rare condition Langerhans cell histiocytosis (LCH), in a case report published on November 24 in the American Journal of Case Reports.
An x-ray of the man's mouth taken a couple years earlier did not show any aggressive alveolar bone destruction or bone loss. The most recent x-ray showed geographic bony destruction of the upper jaw and both sides of the lower jaw "with the teeth appearing to float," highlighting the need to perform these routine scans on patients, according to the authors.
"This case illustrates the importance of orthopantomography (OPG) as a screening tool in new patients to perform an overall evaluation of the teeth and surrounding structures, such as the bone, temporomandibular joint, and sinuses," wrote the group, led by Dr. Amr Bugshan of the Imam Abdulrahman Bin Faisal University College of Dentistry in Dammam, Saudi Arabia.
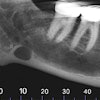
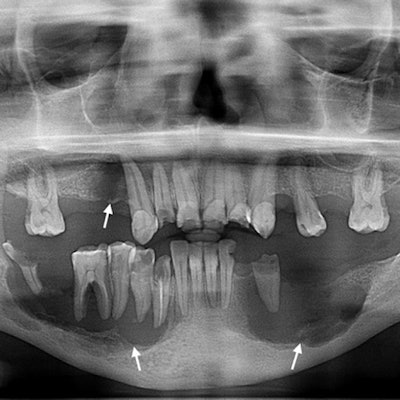
 (A) Orthopantomogram reveals destructive radiolucent lesions in the man's mandible bilaterally and a third lesion distal to the right maxillary canine area. (B) OPG taken two years earlier reveals multiple small, periapical odontogenic lesions in the mandibular left premolars and the right molar. All images courtesy of Bugshan et al. Licensed under CC BY-NC 4.0.
(A) Orthopantomogram reveals destructive radiolucent lesions in the man's mandible bilaterally and a third lesion distal to the right maxillary canine area. (B) OPG taken two years earlier reveals multiple small, periapical odontogenic lesions in the mandibular left premolars and the right molar. All images courtesy of Bugshan et al. Licensed under CC BY-NC 4.0.Rare but serious
Langerhans cell histiocytosis is a rare disorder with abnormal growths resulting from the buildup of Langerhans cells. It presents with a strong inflammatory response and can manifest as a single lesion or with severe multisystem involvement. Up to 20% of cases of LCH occur in the jaw. Early diagnosis of the condition prevents disease progression and may avert further complications.
In the current case, the 42-year-old man went to the dentist because he wanted missing teeth restored. He had no significant medical history and his extraoral findings were unremarkable. A closer look revealed multiple missing teeth, multiple remaining roots, and moderate gingival inflammation with grade III mobility of the mandibular posterior teeth bilaterally, the authors wrote.
An orthopantomogram showed bilateral, well-defined radiolucent lesions eroding the premolar and molar areas of the lower jaw with complete loss of alveolar bone around the back teeth of the lower jaw. The scan revealed that one lesion epicenter was at the midroot level. Another lesion was found on the right upper jaw distal to the canine tooth. The clinicians didn't detect root resorption or displacement. Instead, they found multiple small, periapical tumors that originated from the left premolars and right molar in the lower jaw, compared with OPG performed two years earlier.
A computed tomography (CT) scan showed multiple nonexpansible osteolytic lesions associated with multiple floating teeth on the right anterior upper jaw and bilaterally on the lower jaw. A whole-body CT scan showed increased uptake in both mandibular bodies, extending to the angle of the mandible. A single photon-emission CT (SPECT/CT) scan showed intense localized osseous uptake in the same areas noted on the whole-body scan, the authors wrote.
The patient was diagnosed with LCH due to the location of the lesions in the jaw, the "punched-out" radiolucent density, and the radiographic "floating-in-air" appearance of the teeth. Lab results confirmed the diagnosis of LCH. The man is receiving intralesional steroid injections for mandibular LCH, according to the authors.
 (A) Multidetector CT axial view slices of the maxilla and mandible reveal nonexpansible osteolytic lesions in the upper and lower jaws. (B) Whole-body bone CT shows increased uptake in the mandible. (C) SPECT/CT shows a high rate of metabolic activity in the same regions.
(A) Multidetector CT axial view slices of the maxilla and mandible reveal nonexpansible osteolytic lesions in the upper and lower jaws. (B) Whole-body bone CT shows increased uptake in the mandible. (C) SPECT/CT shows a high rate of metabolic activity in the same regions.
Floating teeth not enough
Although rare, LCH should be considered as a possible diagnosis when orthopantomography shows "floating teeth." In these cases, clinicians also should request full-body imaging to look for lesions in other organs. Additionally, dental x-rays should be used to monitor the development, progress, and aggressiveness of bony lesions of the jaw, they wrote.
"Treating a patient without taking a current dental radiograph that includes OPG can lead to misdiagnosis, delayed diagnosis, and mismanagement," the authors wrote.