A new artificial intelligence (AI) model may provide support for detecting periapical lesions on cone-beam computed tomography (CBCT), according to a study published in the Journal of Dentistry.
Furthermore, the CBCT Segment Anything Model (SAM) may reduce human error and enable early detection of dental pathologies, the authors wrote.
"CBCT-SAM is capable of providing expert-level assistance in the identification of periapical lesions on CBCT," wrote the authors, led by Ka-Kei Chau of the University of Hong Kong (J Dent, December 10, 2024, Vol. 153, 105526).
Since periapical lesions are not always visible on radiographic scans, they may be missed. This occurrence can happen more often with less experienced dentists and when lesions are asymptomatic or are in the early stages. This is particularly true for CBCT scans with a large field of view.
Therefore, this study aimed to evaluate the effectiveness of CBCT-SAM in detecting periapical lesions on CBCT, they wrote.
The study used 185 CBCT scans with confirmed periapical lesions for model training and validation. A trained operator prepared manual segmentation labels, which were validated by a maxillofacial radiologist. The diagnostic and segmentation performance of four AI models were evaluated and compared including CBCT-SAM, CBCT-SAM without the progressive prediction refinement (PPR) module, and two previously developed models, modified U-Net and PAL-Net.
The models' diagnostic performance was evaluated using accuracy based on a binary classification of detected versus missed cases, with correct detection defined as any prediction with a true positive value above zero. Segmentation performance was assessed using five metrics, including accuracy, sensitivity, specificity, precision, and Dice similarity coefficient (DSC), they wrote.
CBCT-SAM achieved an average diagnostic accuracy of 98.92% (± 10.37%) and an average segmentation accuracy of 99.65% (± 0.66%). Its average sensitivity, specificity, precision, and DSC were 72.36% ± 21.61%, 99.87% (± 0.11%), 0.73 (± 0.21), and 0.70 (± 0.19), respectively.
Additionally, CBCT-SAM outperformed modified U-Net in segmentation accuracy (p = 0.023), sensitivity (p = 0.000), and DSC (p = 0.001). While there were no significant differences between CBCT-SAM, CBCT-SAM without PPR, and PAL-Net, CBCT-SAM with PPR outperformed PAL-Net in both diagnostic and segmentation tasks, the authors wrote.
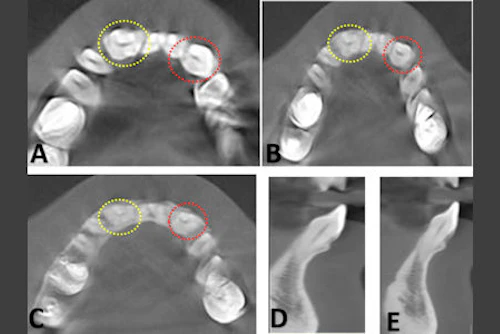
However, the study had limitations, including its small sample size and limited data diversity. Most samples only involved upper and lower posterior periapical lesions, potentially limiting the AI models' applicability across different locations, the authors added.
"Although further modifications and testing are required, it could be a potential tool to provide expert-level assistance chairside to help increase the diagnostic efficiency of inexperienced dentists, reducing the chance of missed diagnosis and facilitating early detection and treatment of initial periapical lesions," they concluded.