Cone-beam computed tomography (CBCT) may not be a dependable tool in assessing alveolar bone loss (ABL) in adolescent orthodontic patients, according to a study published on June 29 in the International Journal of Paediatric Dentistry.
Ultrasound may be a better tool, since it had greater inter and intrarater reliabilities for measuring buccal and labial alveolar bone loss in children than CBCT, the authors wrote. This is believed to be the first study to compare ultrasound and CBCT measurements for adolescent alveolar bone loss.
“Hence, the use of the CBCT procedure for orthodontic treatment in children and adolescents for determining the ABL in the mandibular incisors should be considered with caution due to the limitations outlined in this study,” wrote the authors, led by Dr. Lawrence H. Le of the department of radiology and diagnostic imaging at the University of Alberta in Edmonton, Alberta, Canada (Int J Paediatr Dent, June 29, 2023).
While dental x-rays and CBCT have been mainstays in intraoral imaging, there is increasing concern about the biological effects of ionizing radiation with the use of these modalities. In orthodontics, concerns about radiation exposure are heightened since most of the patients are children.
Intraoral ultrasound, though, is an emerging imaging modality that has advantages over CBCT. It is noninvasive, free of ionizing radiation, portable, and inexpensive. Furthermore, ultrasound can visualize soft tissues, as well as hard dental structures, like the alveolar bone. Additionally, ultrasound has shown high interrater reliability and solid agreement with CBCT alveolar bone loss measurements in adults, the authors wrote.
To compare ultrasound and CBCT as tools for measuring ABL in adolescents undergoing orthodontic treatment, 118 incisors from 30 children underwent imaging. The teeth were scanned by CBCT with 0.3-mm voxel size and with ultrasound at 20 MHz frequency. ABL, which is the distance between the cementoenamel junction and the alveolar bone crest, was measured twice to compare the accuracy of the measurements between the two imaging modalities. Also, the research team compared the intra and interrater reliabilities in measuring bone loss by four raters, according to the study.
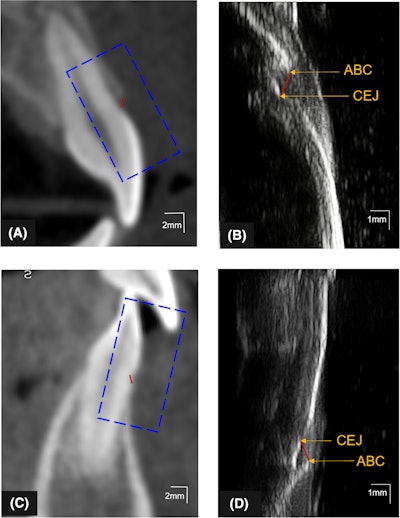
 Illustration of the ABL measurement (red lines) on CBCT and ultrasound images of the (A, B) maxillary and (C, D) mandibular central incisors. The ultrasound images (B, D) correspond to the enclosures (blue-dashed rectangles) and in CBCT images (A, C) of the same teeth with the identified cementoenamel junction and alveolar bone crest. Images courtesy of Le et al. Licensed by CC BY 4.0.
Illustration of the ABL measurement (red lines) on CBCT and ultrasound images of the (A, B) maxillary and (C, D) mandibular central incisors. The ultrasound images (B, D) correspond to the enclosures (blue-dashed rectangles) and in CBCT images (A, C) of the same teeth with the identified cementoenamel junction and alveolar bone crest. Images courtesy of Le et al. Licensed by CC BY 4.0.
For all teeth, the mean difference in ABL between ultrasound and CBCT was -0.07 mm (95% limit of agreement [LoA] of -0.47 to 0.32 mm). For the mandible, the mean differences between ultrasound and CBCT were -0.18 mm (95% LoA of -0.53 to 0.18 mm) and 0.03 mm for maxilla (95% LoA from -0.28 to 0.35 mm), the authors wrote.
In addition, ultrasound had higher intrarater (intraclass correlation coefficients [ICC] = 0.83 to 0.90) and interrater reliabilities (ICC = 0.97) in ABL measurement compared to CBCT (ICC = 0.56 to 0.78 for intrarater reliabilities; ICC = 0.69 for interrater reliabilities), they wrote.
 CBCT images of the incisors with (A) patient motion and (C) the presence of thin alveolar bone. The ultrasound images (B, D) correspond to the enclosures in CBCT images (blue-dashed rectangles) of the same teeth with the identified cementoenamel junction and alveolar bone crest.
CBCT images of the incisors with (A) patient motion and (C) the presence of thin alveolar bone. The ultrasound images (B, D) correspond to the enclosures in CBCT images (blue-dashed rectangles) of the same teeth with the identified cementoenamel junction and alveolar bone crest.
The study had limitations, including that ultrasound was only used on the buccal/labial side of the patient’s teeth due to the size of the transducer. This factor limited intraoral reach, the authors wrote. In the future, studies with larger samples should be conducted on different tooth types to assess bone loss before and after orthodontic treatment, they wrote.
“Ultrasound technology can provide real-time visualization to monitor the ABL and other periodontal structures at repeated visits without the risk of added radiation dose to the individual,” Le and colleagues wrote.