An uncommon 4 x 2.5-cm tumor was removed from a man's hard palate, marking only the fourth documented case of an osteolipoma discovered in this area of the mouth, according to the authors of a case report published May 15 in the Cureus Journal of Medical Science.
Given the extremely rare occurrence of these tumors, they remain unrecognized by clinicians, creating diagnostic problems.
"Osteolipoma should be included as one of the important differentials among the hard palate lesions," wrote Sonam Sharma, MD, and Vikas Dhillon from Kalpana Chawla Government Medical College in Karnal, Haryana, India.
Osteolipoma is a rarely reported variant of a lipoma -- the most common type of benign connective tissue tumor -- that shows bone formation. Finding this type of tumor in the hard palate is very rare, with only three other cases reported in the world. Only 1% to 4% of all benign lesions occur in the oral cavity, and when they do, they grow on the buccal mucosa, tongue, floor of the mouth, lips, and gingiva.
Lipomas can occur anywhere, but they most often grow where fat exists. Because the hard palate has very little fat, the chance of one occurring there is low. It is unclear why lipomas occur, but some evidence links them to genetics and obesity.
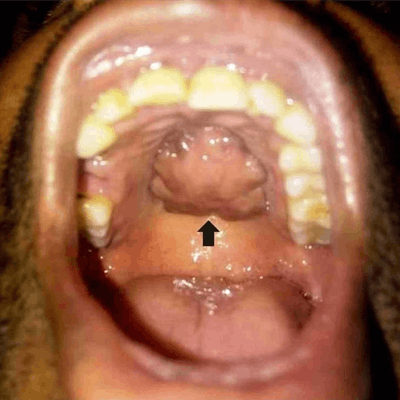
 Hard palate growth upon intraoral clinical inspection. All images courtesy of Sonam Sharma, MD, et al. Licensed under CC BY-NC 4.0.
Hard palate growth upon intraoral clinical inspection. All images courtesy of Sonam Sharma, MD, et al. Licensed under CC BY-NC 4.0.A growing problem
In the current case, a 35-year-old man visited an otorhinolaryngology outpatient department for a painless mass that had been on his hard palate for eight years. It started as a pea-sized mass but gradually grew over the past four years. He had no other oral lesions, pain, bleeding, sensory changes, trauma, or any other symptoms. His past medical and dental histories were unremarkable. He was in good physical health and his vital signs were normal.
An exam of the man's mouth showed that his oral hygiene was poor and that a 4 x 2.5-cm, well-defined, firm, immobile mass was clearly visible on his hard palate, according to the authors.
A CT scan of the face revealed a well-defined, lobulated soft-tissue lesion with a peripheral rim of calcification along the inferior aspect of the hard palate. It did not appear to invade any adjacent structure.
Clinicians suspected the mass could be a calcified hamartoma or an osseous choristoma. Fine-needle aspiration cytology was performed, but no material could be removed from the lesion due its hardness. Because a diagnosis couldn't be established, the man was placed under general anesthesia and the lesion was removed so it could be examined, the authors noted.
The mass was found to be lined by keratinized stratified squamous epithelium. Inside, it had an abundance of mature adipose tissue, as well as variably sized and shaped normal bony partitions. The histopathological exam allowed for the definitive diagnosis of an osteolipoma.
 Figure A is the macroscopic decalcified specimen removed from the oral cavity. Figure B shows the yellow-gray hard cut surface of the tumor.
Figure A is the macroscopic decalcified specimen removed from the oral cavity. Figure B shows the yellow-gray hard cut surface of the tumor.Teaching moment
The CT scan and the needle aspiration procedure did not lead to a definitive diagnosis of the tumor. When this occurs, masses should be surgically removed and examined, they explained.
"A close monitoring and long-term follow-up of such patients is mandatory as the possibility of malignant transformation and recurrence rate of this tumor cannot be commented upon so far due to the scarcity of clinical data available till date," the authors wrote.