A 70-year-old patient presented to the dental practice for an emergency exam after experiencing pain around the peri-implant tissues of implant #5. On evaluation, sulcular pus and buccal edematous tissue were observed -- both associated with the implant in question. Following radiological studies of the affected area, implant #5 exhibited coronal bone loss and classic “cupping,” consistent with signs of occlusal overload. The patient received a diagnosis of peri-implant disease secondary to occlusal overload.
 Above: Preoperative radiograph of the implant on tooth #5. Below: Peri-implant disease is shown around the coronal portion of implant #5. All images courtesy of Dr. Daniel Haghighi.
Above: Preoperative radiograph of the implant on tooth #5. Below: Peri-implant disease is shown around the coronal portion of implant #5. All images courtesy of Dr. Daniel Haghighi.Clinical objective
Because this was a complex case, an extensive treatment plan was developed, and advanced laser technology was used to maximize efficiency, effectiveness, and safety. Treatment consisted of debridement and disinfection with the Solea dental laser (Convergent Dental), a 9.3-µm CO2 laser, with guided bone regeneration.
The clinical objectives were to remove the cause of the disease and then appropriately manage the osseous tissue and soft-tissue defects.
Technique
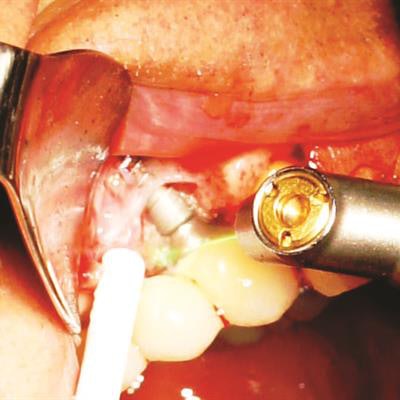
The procedure began with careful ablation of the affected area, which included hard and soft tissues, for several minutes intermittently. The implant surface of #5 was lightly brush-stroked with the laser beam and then the bony defect was forcefully ablated. Laser application was continued until the site was clean and visually free of granulation tissue.
 Above: A full-thickness curvilinear approach was used in this patient. Note both the buccal dehiscence and coronal bone loss. Below: The removal of granulation tissue in bony defect is completed. Bottom: The surgery site is ready for guided bone regeneration.
Above: A full-thickness curvilinear approach was used in this patient. Note both the buccal dehiscence and coronal bone loss. Below: The removal of granulation tissue in bony defect is completed. Bottom: The surgery site is ready for guided bone regeneration.Because of the laser's design, fast and precise cutting was easy to achieve, as ablation only requires adding more (for hard tissue) or less (for soft tissue) pressure to its variable-speed foot pedal. Additionally, the 9.3-µm wavelength allowed for simple removal of the edematous tissue while maintaining the integrity of the tooth. Healthy bone remained, and the implant surface was not significantly altered. The water mist permitted thorough cleaning of the site visually, which aided in predictability.
 Above: Tacks were used to stabilize bone sheet. Below: A platelet-rich fibrin membrane is placed over the secured bone sheet.
Above: Tacks were used to stabilize bone sheet. Below: A platelet-rich fibrin membrane is placed over the secured bone sheet.The patient recovered quickly, and no postoperative complications were observed. The one-year follow-up exam demonstrated an excellent result.
Advantages
When it comes to this type of surgery, most practitioners will agree that it can be both challenging and laborious. Multiple steps have to be performed effectively or the final result could be compromised. However, using the right tool can save a significant amount of time, maximize efficiency, and ensure successful clinical outcomes.
 Above: The full-thickness flap was heavily released for untensioned closure. The prosthesis was placed in implant-protected occlusion, and an occlusal guard was seated six weeks after the procedure. Below: The patient’s mouth immediately after the procedure.
Above: The full-thickness flap was heavily released for untensioned closure. The prosthesis was placed in implant-protected occlusion, and an occlusal guard was seated six weeks after the procedure. Below: The patient’s mouth immediately after the procedure. Periapical radiograph of implant #5 at one-year follow-up demonstrates excellent maintenance of peri-implant coronal bone levels.
Periapical radiograph of implant #5 at one-year follow-up demonstrates excellent maintenance of peri-implant coronal bone levels.Using a CO2 laser has many advantages. For instance, the cumbersome process of scrubbing the implant surface with gauze and then debriding the area with curettes is no longer necessary. This greatly reduces procedure time. This laser also ablates tissue quickly -- even granulation tissue in hard-to-reach crevices. Additionally, it is less invasive than traditional debridement, as the laser helps preserve healthy tooth structure.
Another major advantage of laser dentistry in this case is improved disinfection. With its mist setting at 100%, this laser disinfects the implant surface, keeping it cool. Practitioners will also find that it promotes excellent perfusion from the bony crypt of the defect and bone bed of guided bone regeneration site.
Daniel Haghighi, DDS, owns a private practice in Longview, WA. He is a founding partner of Surgikor Implants.
The comments and observations expressed herein do not necessarily reflect the opinions of DrBicuspid.com, nor should they be construed as an endorsement or admonishment of any particular idea, vendor, or organization.



















