A handheld device that uses electronic impedance spectroscopy to measure a tooth's mineral density and detect caries is now making its way into the U.S. market, and its developers say it yields fewer false positives and greater accuracy than competing laser fluorescence products.
“Specificity is where we're different and we blow everybody away.”
— Rich Gresser, vice president of
sales, CarieScan
The CarieScan Pro, which was developed in Scotland using technology from the universities of St. Andrews and Dundee, was originally introduced in 2007 and received FDA clearance in December 2009. In July, CarieScan -- a wholly owned subsidiary of 3D Diagnostic Imaging -- signed an exclusive U.S. distribution agreement with Patterson Dental, and last month the company opened its first U.S. headquarters in North Carolina.
CarieScan is now gearing up to challenge the existing caries-detection products on the market, which include the Diagnodent and Midwest Caries ID. The device will sell for $3,995 in the U.S.
"We believe that CarieScan Pro is an essential device for progressive dentists and hygienists who value prevention," said Graham Lay, CEO, in a press release announcing the company's deal with Patterson.
How it works
The concept of using electrical signals for caries detection dates from the 1950s, the company said, noting that the Vanguard fixed frequency electrical caries monitor was used in U.S. dental practices during the 1970s. In the early 1980s, a similar Japanese device, the Caries Meter L, was also available commercially. And in the 1990s, a Dutch meat-processing company produced a copy of the Vanguard device, the ECM, that showed promising results, according to CarieScan.
 The CarieScan Pro caries detection device. All images courtesy of CarieScan.
The CarieScan Pro caries detection device. All images courtesy of CarieScan.
In 1996, Nature Medicine (February 1996, Vol. 2:2, pp. 235-237) reported on the first use of multiple electrical frequencies involving a method known as AC impedance spectroscopy technique (ACIST). The use of variable frequencies was a major step forward in characterizing the status of dental hard tissues more accurately and being able to better differentiate between healthy and diseased teeth, according to CarieScan.
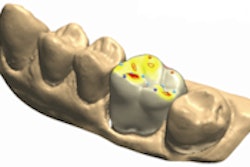
ACIST uses alternating low-voltage electrical current to pass through tooth enamel into the pulp, explained Rich Gresser, vice president of sales at CarieScan. The CarieScan system then assigns mapped values from 1 to 100 based on electronic impedance, taking into account more than 200 values measuring the peaks of electrical current. CarieScan's display readings show numerical values from 1 to 100 (1 being normal, 100 requiring operative procedures), accompanied by color bars ranging from green (initial carious changes) to red (established dentinal caries).
"The process measures tooth mineral density or porosity of the entire tooth," Gresser told DrBicuspid.com. "It goes through the entire tooth; it doesn't just scan the surface."
The variance in signals between the different stages of decay is significant, according to CarieScan. The impedance measured in a healthy tooth is significantly greater than that of a tooth that is demineralizing, which is itself significantly greater than that of a tooth with a carious lesion. As a result, the sensitivity and specificity of the ACIST technique in distinguishing these different stages are very high.
Clinical research
Several clinical studies have demonstrated the viability of ACIST for accurate caries detection, CarieScan noted.
For example, a 1996 study in the Journal of Dental Research (November 1996, Vol. 75:11, pp. 1871-1878) concluded that "electrical impedance spectroscopy, measuring impedance over a large range of frequencies, will provide more detailed information about the electrical characteristics of teeth. It is concluded that the in vitro performance of electrical impedance spectroscopy in differentiating among sound, noncavitated carious, and cavitated approximal tooth surfaces is excellent."
Similarly, a 1998 study that compared ECM with visual examination, fiber-optic transillumination, and conventional and digital bitewing radiography concluded that "ECM was the most accurate diagnostic tool for the in vitro diagnosis of early, noncavitated occlusal lesions on posterior teeth" (Journal of Dentistry, March 1998, Vol. 26:2, pp. 83-88).
More recently, a study in Caries Research demonstrated that an ACIST device can be optimized to aid caries detection and monitoring by displaying results with symmetrically high values for both sensitivity and specificity (May 2008, Vol. 42:3, pp. 185-238). And a presentation at the 2008 International Association for Dental Research meeting showed that the electrical impedance device was able to detect 31% of all the hidden dentine lesions not detected by optimal clinical visual assessment and 100% of deep hidden dentine lesions.
Fewer false positives
CarieScan contends that while fluorescence-based systems are effective in finding established dental lesions and caries better than conventional visual and radiographic methods, they are prone to a high number of false positives, particularly in the presence of staining.
Conversely, CarieScan's ACIST technique produces better specificity of tooth structure and greater accuracy, Gresser said. In fact, the company claims a 93% accuracy rate.
"If caries are there, laser fluorescence will detect it, but specificity is where we're different and we blow everybody away," he said. "There's very little chance of false positives."
The poor specificity associated with laser fluorescence systems can result in false positives readings as high as 40%, which can in turn lead to unnecessary drilling of healthy teeth, Gresser added.
"There's been a huge increase in single surface restorations," he said, resulting in greater scrutiny of claims by insurance companies.
That can expose dentists to liability, Gresser noted. "You don't want to have to tell the patient that you numbed them up and opened up a perfectly healthy tooth," he said.
Copyright © 2010 DrBicuspid.com