They're cheaper. They're easier. They're government-approved. And manufacturers are promoting them heavily. But can mini-implants do everything standard ones can?
Probably not. That's the consensus of top implant experts interviewed by DrBicuspid.com. While the mini-implants (AKA "small-diameter") work better for some purposes, standard implants still win out in lots of others.
Reports about mini-implants -- less than 3 mm in diameter -- are burning up the dental forums. "They do work," one dentist announced on the Osseonews forum recently. "Your expectations will be tempered by a new rash of failed cases," another shot back.
The truth lies somewhere in between, according to Ken Judy, DDS, co-chair of the International Congress of Oral Implantologists and a clinical professor of oral implantology at New York University. He recommends using small implants for the following:
- Stabilization of a prosthesis
- Cases in which there isn't enough space between teeth or implants for a standard diameter implant
- Some circumstances in which the patient wants to save money
An extra-small implant can support nice-looking overdentures, and for the cost-conscious patient, that may be enough. In some cases, patients can save tens of thousands of dollars by avoiding the surgery required to expose bones and place standard implants, Dr. Judy said. Unlike standard implants, minis can often be placed straight through the gum.
But in most cases, he'd rather install the standard size. "What most patients want are teeth that are permanent, nonremovable, porcelain, and beautiful," he said. "You can't provide [a set of] permanent teeth with mini-implants."
With smaller implants, some experts say, the key is using them only where they will experience minimal stress. "It's like putting a stick in the ground and trying to support something on it," said Michael P. Rethman, DDS, past president of the American Academy of Periodontology and an adjunct faculty member at the University of Maryland. "If you just want to put a sign on it that says, 'Welcome to my son's first birthday,' that's just fine. If you want to put a car on it, that's another matter."
Mini-implants are nothing new. "They just became very popular for denture stabilization," Dr. Judy explained. Patients who walked into a dentist's office with loose dentures didn't want to wait months for a standard implant to be ready for loading. The solution many dentists tried was placing standard implants and mini-implants at the same time. The mini-implants were intended to hold the overdentures in place while the standard implants osseointegrated.
When dentists using this approach saw their patients a few months later -- planning to attach the dentures to the standard implants -- they discovered the mini-implants had osseointegrated, too.
When this discovery was confirmed by histology, dentists realized that extra-small implants might serve a permanent purpose. In 2003, the U.S. Food and Drug Administration approved mini-implants by IMTEC for long-term use, defined as longer than two years. In 2004, the agency approved mini-implants from Dentatus, and from Intra-Lock this year, with other brands headed down the pipeline.
So how well do the mini-implants work?
The jury is still out, said Robert Chapman, DDS, chair of prosthodontics and operative dentistry at Tufts University. "There's anecdotal information that they may be helpful. But the ones smaller than 3.0 mm have no good data I was able to find."
As for length, "anything under 8 mm appeared to have a lower success rate," he said.
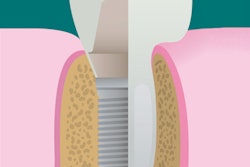
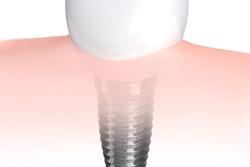
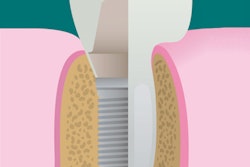
 |
| A mini dental implant (MDI) made by IMTEC. Image courtesy of IMTEC. |
Not surprisingly, what Dr. Chapman called his "nonrecommendation" doesn't sit well with Bernard Weissman, president of Dentatus, who invented implants for the company with diameters as narrow as 1.8 mm. "He doesn't know what he's talking about," said Weissman, whose company supplied DrBicuspid.com with two case reports and five longitudinal studies on the company's narrow implants. Two of the longitudinal studies appeared in peer-reviewed journals; the rest were presented at professional meetings.
The most impressive report was published in the International Journal of Periodontics & Restorative Dentistry in September/October, 2007. In it, researchers retrospectively analyzed data on 48 implants ranging from 1.8 mm to 2.4 mm in diameter, placed in 27 patients. After one to five years, none of the implants had failed.
The results are encouraging, but as the authors concluded, "evaluation of these NDIs [narrow-diameter implants] for long-term use will require additional multicenter prospective longitudinal studies."
Responding to a similar query from DrBicuspid.com, IMTEC produced a December 2005 article from Compendium of Continuing Education in Dentistry reporting on 1,029 implants used to support prostheses. These implants, also ranging from 1.8 mm to 2.4 mm in diameter, had a survival rate of 91.17% after five months to eight years. Zeroing in on 62 of the mini-implants that were in place for more than five years, the investigators found that 55 (88.7%) had survived. "This information suggests that mini-implants can be effective devices for use in long-term denture stabilization," the researchers concluded. (A subsequent article in the same journal had even more impressive results.)
To date, though, it appears that no researcher has tried a randomized head-to-head face-off between small-diameter implants and standard-sized ones in situations where either might be used.
And all these studies looked at small-diameter implants. What about short ones? Actually, the two dimensions should be considered together, according to the authors of a review published in the October 2007 Journal of Oral Implantology. In the posterior maxilla, where bone height is low, a short implant (down to 5.75 mm in length) can take the place of a standard-length implant, provided the shorty is also a fatty, they write.
The key, the authors explain, is osseointegration, which (assuming the implants are of the same material) depends on surface area. "The use of a 5-mm-diameter implant that is 6-mm long increases the surface area available to contact the bone similar to that of a 3.75-mm-diameter implant that is 10 mm in length," they write. Also, they found, the implants with a rough surface integrate better than those with machined surfaces.
Another possibility: "You can make up for [length] by increasing the number of implants," Dr. Judy said.
Others have proposed a similar rule for narrow diameters; where possible, use more implants.
Dr. Judy argued against using mini-implants to replace individual wide teeth (for example, maxillary central incisors) or for patients with especially muscular jaws.
Dr. Judy also recommendsed that a general dentist getting into implants take a course of at least 12 days from a university or independent institute -- such as those listed on the website of the International Congress of Oral Implantologists.
One risk for a general dentist taking a course from a company that makes mini-implants is that you won't learn how to do standard implants as well. "That's a concern," Dr. Judy said. "It's like carpentry. If you only train to use nails, then all you ever use is nails. Screws and bolts, you'll never use."