A giant calcified salivary stone, which was diagnosed initially as an impacted tooth, was recently found growing in the mandible of a 37-year-old man. A rare 2-cm-long sialolith was removed, according to a new case report.
Any salivary stone that is larger than 1.5 cm is considered rare, according to the authors of the report, published in BMJ Case Reports (February 28, 2020). In this case, the appearance of a giant sialolith on an orthopantomogram, resembling an impacted supernumerary tooth, led to misdiagnosis, they noted.
"Such presentation is rare," wrote the authors, led by Kumar Nilesh, MDS, of the department of oral and maxillofacial surgery at Krishna Institute of Medical Sciences in Karad, India.
How it unfolded
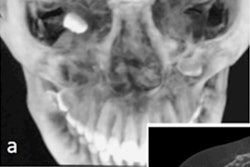
The man was referred to an oral surgeon to have an impacted tooth treated after experiencing intense swelling and pain. An orthopantomogram of the patient showed both jaws with normal teeth. Horizontally impacted mandibular third molars were seen. A linear radiopacity was detected, extending coronally between teeth #44 and #45 and extending apically below the roots of tooth #46, resembling an impacted supernumerary tooth, according to the authors.
Ultrasonography was performed for better imaging of the soft-tissue swelling. Upon closer review, the clinician was able to see that the patient had a 2-cm-long sialolith instead of an impacted tooth, the authors wrote.
After the discovery, the patient was placed under general anesthesia, and the giant salivary stone was removed via the submandibular duct opening. Absorbable sutures were used to close the wound. When the patient was evaluated during a follow-up visit after the surgery, clinicians found that he had healed without problems and his pain and swelling was gone, according to the case report.
Avoiding misdiagnosis
Misinterpreting the finding of a linear radiopacity mimicking an impacted tooth on an orthopantomogram is highly unusual. To differentiate between a sialolith and an impacted tooth on orthopantomogram, clinicians should look for a lack of sclerotic margins of lamina dura, absence of radiolucent central pulp chamber, and differential radiolucency between enamel and dentin. Clinicians also should consider using other types of diagnostic tools, the authors wrote.
"Use of correct diagnostic aid, like USG [ultrasonography], helps in arriving at [the] correct diagnosis, thus avoiding wrong treatment," they wrote.