|
To some, endodontics is a fascinating process. Techniques can be debated and argued, with each professional making their own decision on what works best for them and their patients. This issue of THE DENTAL ADVISOR (July-August 2008, Vol. 25:6) discusses new products designed to improve the endodontic experience and present comparative properties of gutta-percha and Resilon, NiTi rotary files, and endodontic handpieces. Contributing authors: Santine Anderson, D.D.S.; Robert Stevenson, D.D.S.; William T. Stevenson, D.D.S.
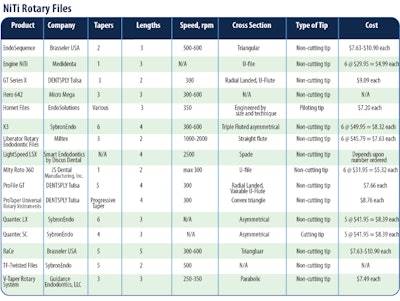
Product Comparison Charts (Click links below to view)Endodontic Obturation Devices Endodontic Ultrasonic Systems NiTi Rotary Files Gutta-Percha and Resilon
One of the primary goals of endodontic therapy is to obtain a complete, three-dimensional obturation of the canal system. The filling material should be dimensionally stable, nontoxic, and easy to place. Gutta-percha, a natural material, has been the obturation choice since its introduction. Relatively new on the market is an obturation alternative called Resilon by Resilon Research, LLC. Resilon is a synthetic polymer of polyester, methacrylate resin, bioactive glass, calcium hydroxide, and various radiopaque fillers. The sealer bonds to the root structure via a methacrylate resin adhesive. Resilon is available as Epiphany, Pentron Clinical Technologies; RealSeal, SybronEndo; SimpliFil, Discus Dental; and Resinate, Obtura Spartan. To completely fill the canal, methods have been devised to soften the gutta-percha with heat and then compact the material into the canal. These methods soften the gutta-percha or Resilon before insertion in the canal, heat the material during placement, or supply heat to the gutta-percha within the canal space. Both are also delivered via heated or injection systems to soften the filling material in the canal. Each material has individual benefits, but each shares the need for an adequately shaped canal that allows placement and condensing of the obturation material. A sealer is recommended for use with all of the obturation systems. Some fast-set sealers exhibit accelerated setting times when used with thermoplasticised gutta-percha or Resilon and are not recommended. The use of sodium hypochlorite and peroxide-based lubricants are essential to cleaning and shaping of the root canal but may affect the bond of Resilon to the canal or the setting of the material in the canal. To counteract this effect, use EDTA followed by sterile water as the last step during irrigation. Chlorhexidine does not affect the bond strength and may be placed before the primer. NiTi Rotary Files
NiTi rotary instruments utilize a superelastic, nickel-titanium (NiTi) alloy that permits the instruments to be rotated in curved canal systems. A very light touch must be used, keeping the handpiece at a constant speed within the canal. Manufacturers of NiTi rotary instruments claim various advantages due to the cross-sectional geometry or the number of instruments required or the manner in which their instruments are used. Attention to canal anatomy and recognition of the difficulty in negotiating a particular canal will avoid breakage of an instrument. Clinical Tips
Ultrasonic Usage in Endodontics
Many practitioners prefer piezo electric ultrasonics, as compared to magnostrictive units for endodontic procedures for two main reasons. Piezo electric technology offers more cycles per second (40,000 cps versus 24,000 cps). Also, the tips of these units work in a linear back and forth effect, versus the figure 8 or elliptical motion that magnostrictive units use. This former motion is ideal for endodontics, particularly when "troughing" the pulpal floor for hidden canals. Traditionally dentists have believed that ultrasonic use in endodontics only has a surgical application. There are a growing number of practitioners who are using ultrasonics for nonsurgical endodontic procedures such as finding hidden canals, increasing the efficacy of the irrigation agents, removing posts and cores, and removing separated instruments. Finding Hidden Canals
Piezo electric ultrasonics are excellent for removing the secondary dentin that often slopes off the mesial wall, which is what blocks the MB-2 canal in maxillary molars. Ultrasonics allow for slight removal of tooth structure without compromising the visual field. Ultrasonics also perform particularly well when breaking through the calcification that covers the canal orifice. A good tip to remember when searching for hidden canals is that secondary dentin is generally whitish or opaque, while the floor of the chamber is darker and more gray-like in composition. A fiberoptic on an ultrasonic can assist in visual identification of secondary dentin. Increased Efficacy of the Irrigation Agent
The cleaning efficacy can be enhanced by placing an ultrasonic tip into the irrigated space of the canal. Ultrasonics create both cavitation and acoustic streaming. The cavitation created is minimal and is restricted to the tip. However, the acoustic streaming effect is significant. These motions allow cleaning and flushing out of areas that files may not be able to negotiate. Removing Posts and Cores
Piezo electric ultrasonics are a tremendous help in post removal and are often safer to use than post removal kits. When removing a post, it is critical to break the seal between the post and the tooth structure. This can be accomplished initially through the use of a surgical length ¼-round bur, making sure you are along the long axis of the post. After creating a groove around the post, place an ultrasonic tip into the trough. Using a low setting and copious water will allow breakage of the seal between the tooth and post. Patience is always recommended when removing posts from canals. Removing Separated Instruments
Piezo electric ultrasonic units are also excellent for removing separated instruments. However, you must be aware of the importance of the location of the separated file. If a rotary file is separated past the canal curvature, it will be extremely difficult to remove. When removing a broken instrument in the coronal third of the tooth, a thin spreader tip will work nicely. Most ultrasonic manufacturers have tips specifically designed to remove broken instruments. The tip should be inserted into the canal and moved in a counterclockwise motion around the broken fragment. This technique will generally dislodge the broken instrument. Instruments separated in the middle or apical third of a canal are best removed by an experienced clinician with the use of a microscope. Requests for reprints should be directed to The Dental Advisor. |