A new study that compared the Isolite illuminated isolation system (Isolite Systems) and a saliva ejector for reducing aerosols and spatter during and after ultrasonic scaling found that the best results still come from high-velocity air evacuation (Journal of the American Dental Association, January 2015, Vol. 146:1, pp. 27-33).
The authors found that a significant amount of contamination occurred during ultrasonic scaling, which neither the isolation system nor the saliva ejector reduced effectively. The saliva ejector, which is significantly lighter and easier to maneuver, is the preferred device of dental hygienists, they added.
The high-volume evacuator is the only high-velocity air evacuation device currently available; however, it can be bulky and difficult to maneuver, the study authors noted. The Centers for Disease Control and Prevention (CDC) and the ADA recommend that high-velocity air evacuation and proper patient positioning be used during procedures that produce high amounts of aerosols and spatter.
Study author Jessica Holloman, RDH, program director for Innovations in Interprofessional Oral Health at Northeastern University in Boston, told DrBicuspid.com that she decided to do this research after teaching dental hygiene students to use the high-volume suction while ultrasonic scaling, which is difficult to maneuver when working on your own with a patient.
“I was hoping that the Isolite system would be a good alternative.”
"I was hoping that the Isolite system would be a good alternative, since it allows for hands-free dentistry," she said.
"To my knowledge, the Isolite system has not been studied regarding aerosol and spatter reduction in a clinical environment," she added.
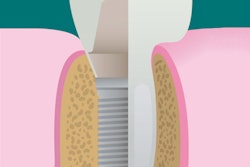
The Isolite illuminated dental isolation system was introduced to the commercial market in 2005 and is designed to attach to the high-volume suction hose, providing simultaneous suction to both maxillary and mandibular quadrants.
For their clinical trial, Holloman and colleagues tested the effectiveness of the Isolite suction device and used the standard saliva ejector as a control. The study was conducted in a single, enclosed dental operatory and microbiological laboratory at the University of North Carolina at Chapel Hill School of Dentistry.
They included 50 participants, who were randomized to either the test device or control group. The study participants were seated in a supine position and received a prophylaxis treatment with an ultrasonic scaler by a licensed dental hygienist with five years of clinical experience and three years of experience with the test device.
To collect aerosols and spatter, the researchers used 20 mL of a sterile liquid transport buffer: Dulbecco phosphate-buffered saline (DPBS) solution. A single petri dish containing the 20 mL of sterile DPBS solution was placed 6 inches from the oral cavity. At the start of ultrasonic scaling, the lid to the petri dish was removed and closed immediately after exposure to the ultrasonic scaler.
It was then replaced with a second petri dish containing 20 mL of fresh DPBS. The second petri dish remained open for 35 minutes to collect postexposure aerosols. The aerosols were collected, dispersed, and plated to anaerobic blood agar to determine colony-forming units (CFUs). The authors did not find a statistically significant difference in aerosol and spatter reduction between the test and control groups. Similarly, the study results found no statistically significant difference between the two groups in CFUs collected in the postexposure period.
However, the researchers did find a sharp decline in CFUs collected after ultrasonic scaling in each group. The most prominent type of bacteria identified was α-hemolytic streptococci, present in 100% of the samples.
"Our study results indicated that there was no statistically significant difference between the two groups in the mean number of CFUs collected during ultrasonic scaling," the authors wrote. They added, however, that the amount of contamination taking place during ultrasonic scaling, as indicated by high bacterial counts in both groups, is of concern.
"We hypothesize that, because our study was the first, to our knowledge, to evaluate the Isolite device with regard to aerosol and spatter reduction in an actual clinical environment, the addition of other variables (plaque, saliva, patient, and operator positioning) contributed to dissimilar findings," they wrote.
Holloman expressed surprise at these findings and said that she expected to find a greater amount of aerosol and spatter reduction. Before using devices that create large amounts of aerosols and spatter, it is imperative to consider how to best reduce them and reduce the bacterial load before beginning treatment, she noted, listing proper patient positioning, toothbrush prophylaxis prior to instrumentation, use of an antimicrobial rinse, proper suction devices, and proper air ventilation as examples.
Neither the Isolite device nor the saliva ejector effectively reduced aerosols and spatter during ultrasonic scaling, indicating that additional measures should be taken to reduce the likelihood of disease transmission, the authors noted. They recommended that clinicians follow the guidelines set by the CDC and the ADA.
Rolando Mia, VP of sales and marketing at Isolite Systems, told DrBicuspid.com that the company has been an advocate of effective isolation for 14 years and the fact that their system was recognized and studied is an acknowledgement of that commitment.
Mia added that when the system was requested, the company did not get a chance to train the participants on the most effective way to use it so as to reduce spatter and aerosols. He also expressed some concern about the structure of the study in terms of baseline data and how the spatter and aerosols were measured.
"When you look at aerosols and spatter, it is important to consider the baseline of what is already in the air," he said. "This needs to be considered to compare."
"We are thrilled that the study is bringing attention to this topic, because it is important for both patient and dental staff safety," he added. "While we appreciate the procedure they used in this study, we hope to do another study with even more rigor about effective isolation during these procedures."
This study was funded, in part, by Isolite Systems.