
Parotid gland abscesses caused unusual facial nerve palsy in two patients, according to a case report published on July 30 in the International Journal of Surgery Case Reports. Only 15 other cases of parotid abscess-induced facial palsy have been reported, the authors noted.
The abscesses occurred in a 75-year-old and an 81-year-old woman. Though clinicians successfully treated both patients, neither woman experienced facial nerve improvement, the authors wrote.
"Facial nerve palsy is rarely caused by parotid abscess," wrote the group, led by Dr. Ineke Pruijn from the department of otorhinolaryngology and head and neck surgery at Radboud University Medical Center in Nijmegen, Netherlands.
75-year-old woman with rapidly swelling neck
A 75-year-old woman went to a hospital's outpatient clinic because she was experiencing painful, rapidly growing infra-auricular swelling for two weeks that extended into the left side of her neck. The woman smoked, drank alcohol regularly, had high blood pressure, and used anticoagulant therapy for atrial fibrillation. She had no other signs of illness other than dry mouth and pain when swallowing foods or liquids, the authors wrote.
 (A) An image of the 75-year-old woman when she presented at the hospital with painful infra-auricular swelling that extended to her neck. (B) The woman, who was treated for a parotid abscess, when she was discharged from the hospital following a 15-day stay. (C) The patient four months after her procedure. All images courtesy of Pruijn et al. Licensed under CC BY-NC-ND 4.0.
(A) An image of the 75-year-old woman when she presented at the hospital with painful infra-auricular swelling that extended to her neck. (B) The woman, who was treated for a parotid abscess, when she was discharged from the hospital following a 15-day stay. (C) The patient four months after her procedure. All images courtesy of Pruijn et al. Licensed under CC BY-NC-ND 4.0.A physical exam revealed an infra-auricular mass that was red and swollen on her left side. When clinicians touched the mass, pus discharged from the opening of her left parotid duct. After the exam, the team collected swabs, and a nerve exam showed the woman was experiencing no signs of facial palsy. A computed tomography (CT) scan revealed a 6.2 x 5.9 x 6.7-cm mass at the left of the parotid gland, which was suspected to be an abscess, they wrote.
The clinicians gave the woman intravenous antibiotics and completed a fine-needle aspiration cytopathological (FNAC) evaluation. The FNAC diagnosed the woman as having a purulent infection without signs of malignancy, the authors noted.
After five days of antibiotics, the woman developed an ipsilateral facial nerve palsy. Her infection also had not improved. Another CT scan showed progression of the mass and further subcutaneous infiltration, so her clinicians referred her to a hospital.
Another physical exam confirmed the infra-auricular mass, which extended retroauricular and down her neck. Otomicroscopic evaluation of her left ear showed destruction of the canal floor, which is where pus discharged when she chewed.
Due to the observed facial nerve palsy and bone destruction, clinicians suspected malignancy of the parotid gland. The team ordered a magnetic resonance imaging (MRI) scan, which showed a large necrotic mass of 5.8 x 4.8 x 7.3 cm extending from the superficial lobe of the woman's left parotid gland to her external ear canal, cutis, temporomandibular joint, and lower neck, confirming she had a parotid abscess, according to the report.
To ensure there was no malignant disease, clinicians performed deeper biopsies of the parotid gland. The retroauricular skin defect revealed a tense capsule on top of the swollen gland. The capsule was incised, and a large quantity of pus was released. A drain was placed at the surgical site so it could be flushed daily, the authors wrote.
Lab results came back positive for Staphylococcus aureus, so her antibiotics were changed. Testing of the samples from the deeper biopsies showed she had a necrotic infection without signs of malignancy or a benign parotid tumor.
Follow-up MRI scans showed a healed cutaneous tissue defect, parotid gland atrophy, and no indications of malignancy. A year after her treatments, the woman's facial nerve palsy had not improved, the authors noted.
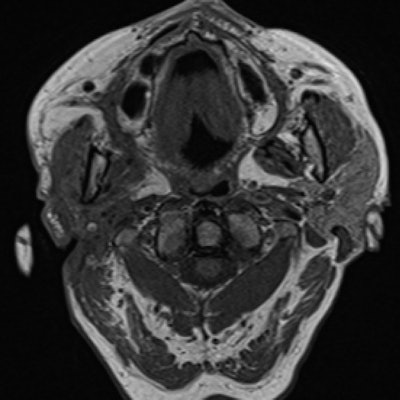
 The 75-year-old woman's head and neck MRI scan showed a healed cutaneous tissue defect, parotid gland atrophy, and no signs of malignancy.
The 75-year-old woman's head and neck MRI scan showed a healed cutaneous tissue defect, parotid gland atrophy, and no signs of malignancy.81-year-old woman with painful swelling
In another case, an 81-year-old woman visited a hospital's outpatient clinic because she had painful, preauricular swelling on her right side. The woman had hypertension, type 2 diabetes, atrial fibrillation, and mild renal impairment.
An intraoral exam showed purulent discharge from the opening of her parotid gland, but she had no signs of facial nerve palsy. Clinicians took swabs of the discharge for analysis, which tested positive for methicillin-resistant S. aureus (MRSA). They gave the patient antibiotics and discharged her.
 (A) An image of an 81-year-old woman when she presented at the hospital with painful preauricular swelling on her right side. (B) The woman, who was treated for a parotid abscess, after all drains were removed. (C) The patient three months after her procedure.
(A) An image of an 81-year-old woman when she presented at the hospital with painful preauricular swelling on her right side. (B) The woman, who was treated for a parotid abscess, after all drains were removed. (C) The patient three months after her procedure.The antibiotics initially helped, but the woman's swelling soon returned. Five days later, she could not shut her right eye. She experienced no other symptoms, such as pain, dizziness, or purulent discharge from her ear.
Further physical examination showed she had facial nerve paralysis on her right side. Later, her preauricular swelling ruptured spontaneously, causing a purulent discharge to evacuate. At that time, she was referred to the hospital for further tests and treatment possibilities.
A hospital physician confirmed that she had a preauricular mass of about 6 x 8 cm extending to her upper neck. Her skin was red and had several ulcers, and her facial nerve paralysis was confirmed. A routine nasopharyngolaryngoscopy revealed a parapharyngeal bulging on the right side, accompanied by a slight uvula shift to the left.
The woman underwent a CT scan that showed a swollen right parotid gland in the parapharyngeal space expanding toward the cutis and the palatine tonsil, with tapering of the internal carotid artery and the presence of subcutaneous infiltration, which suggested a deep parotid abscess, they wrote.
 The 81-year-old woman's head and neck MRI showed no signs of malignancy.
The 81-year-old woman's head and neck MRI showed no signs of malignancy.Clinicians surgically drained the abscess and multiple pus pockets. They then left drains that could be flushed daily and gave the woman intravenous antibiotics.
Two months after treatment, an MRI scan showed volume loss of her parotid gland and no signs of malignancy. Six months after treatment, the woman's facial nerve still had not improved. The patient was scheduled to undergo implantation of a gold-weighted implant in her upper eyelid to treat her persistent open eye caused by facial nerve paralysis.
Rare cases
Facial nerve palsy, along with a preauricular mass, are usually signs of a primary salivary gland malignancy or metastasis in the parotid gland. Evidence suggests that parotid abscesses are an extremely rare cause of facial nerve palsy or paralysis but should not be ruled out when imaging shows no malignancy.
Most frequently, a parotid abscess is caused by acute bacterial parotitis. Factors such as diabetes, poor oral hygiene, and autoimmune diseases may predispose individuals to parotid gland abscesses.
"Facial nerve palsy or paralysis caused by benign parotid gland pathology is rare, especially in the case of a parotid abscess," Pruijn and colleagues wrote.



















